Your Annual Checkup Isn't Built for Women's Hormones
Written By
Suresh Veerapaneni
Founder, Healthvizor

If you're a woman in urban India, your hormonal life probably runs something like this: PCOS or PCOS-like symptoms in your 20s and early 30s; perimenopause beginning quietly in your late 30s or early 40s, long before anyone names it; and menopause itself somewhere around 46–47, several years earlier than the Western average of 51⁹. Because an Indian woman who reaches menopause can expect to live nearly three decades beyond it, what happens to your metabolism, heart, bones and muscle in this transition isn't a footnote. It's most of your adult life.
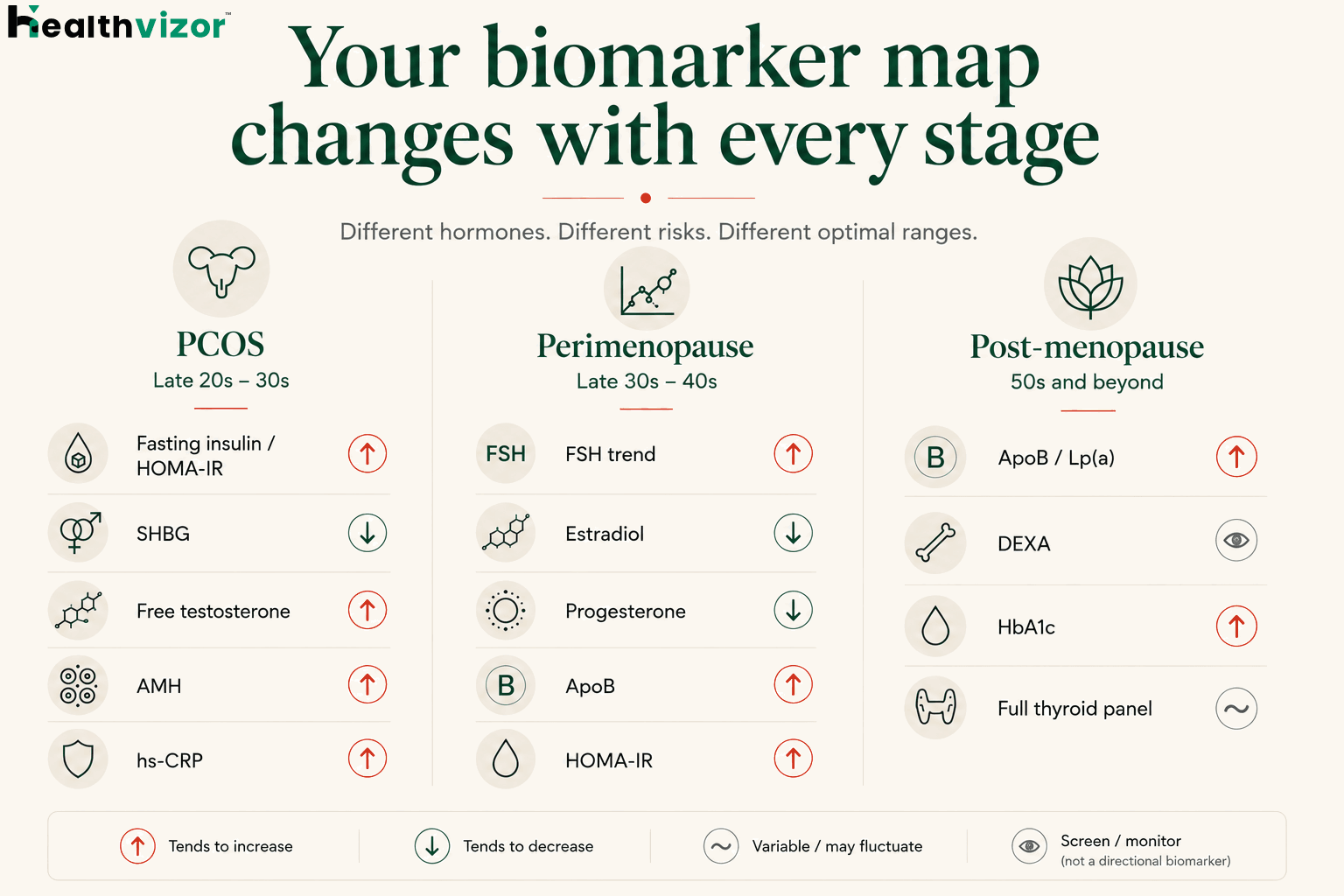
Stage 1: PCOS (and PCOS-like patterns)
PCOS is one of the most common endocrine disorders in women of reproductive age, with insulin resistance present in an estimated 50–70% of cases, in lean and higher-weight women alike, though it's more pronounced with excess weight¹. The 2023 International Evidence-Based Guideline reframed PCOS as not just a reproductive disorder but a metabolic and cardiovascular one¹. That shift matters: it moves the conversation from "get periods regular" to "manage insulin, inflammation and long-term cardiometabolic risk."
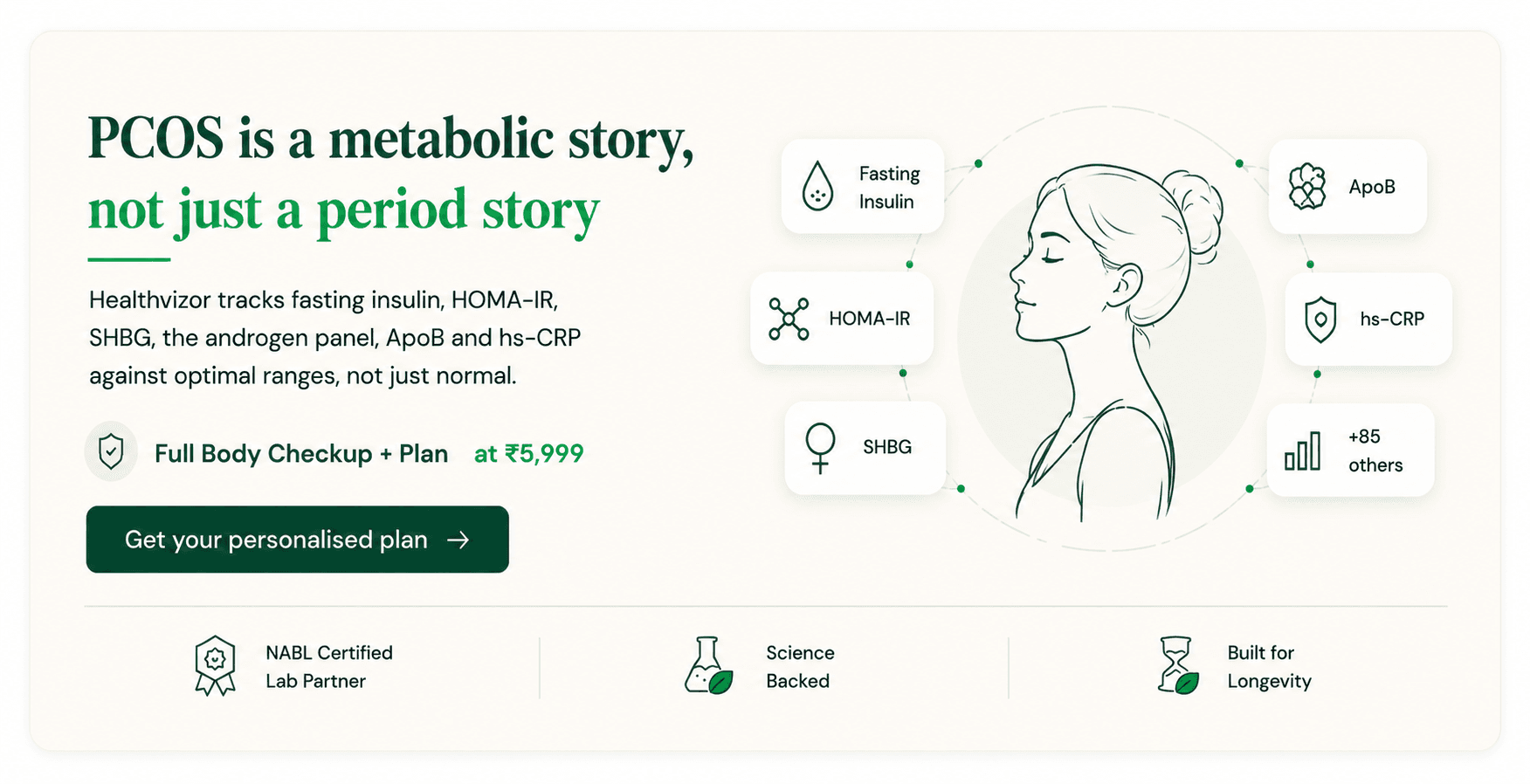
Biomarkers worth tracking
HbA1c: slower-moving; read it as a trend, not a single value.
SHBG: low SHBG is a classic PCOS pattern and tracks with hyperandrogenism.
Total and free testosterone, DHEA-S: the androgen panel.
LH and FSH: useful in context, but not diagnostic on their own.
AMH: often elevated in PCOS. The 2023 guideline now accepts AMH as an alternative to ultrasound for the "polycystic ovary" feature in adults, but it's one piece of the picture, not a stand-alone PCOS test.
Lipid panel + ApoB: PCOS is independently linked to atherogenic lipid patterns.
Vitamin D, B12: commonly low and worth correcting; vitamin D may modestly help insulin sensitivity.
TSH and free T4: rule out a thyroid contribution to weight and cycle issues.
hs-CRP: low-grade inflammation is part of the syndrome.
What the evidence says about management
The 2023 guideline is clear that lifestyle is the foundation: diet, structured exercise and sleep produce real metabolic improvement, with no single "best" diet as long as overall quality and energy are managed¹. Metformin has the strongest evidence of any drug adjunct, meta-analyses show it lowers HOMA-IR, fasting glucose and BMI more than placebo, and it's especially useful at higher BMI². Inositol (myo + d-chiro) has smaller but supportive evidence and is well tolerated. Fertility care deserves its own clinical visit; this article is about the metabolic and cardiovascular side, where most Indian women's PCOS care falls short.
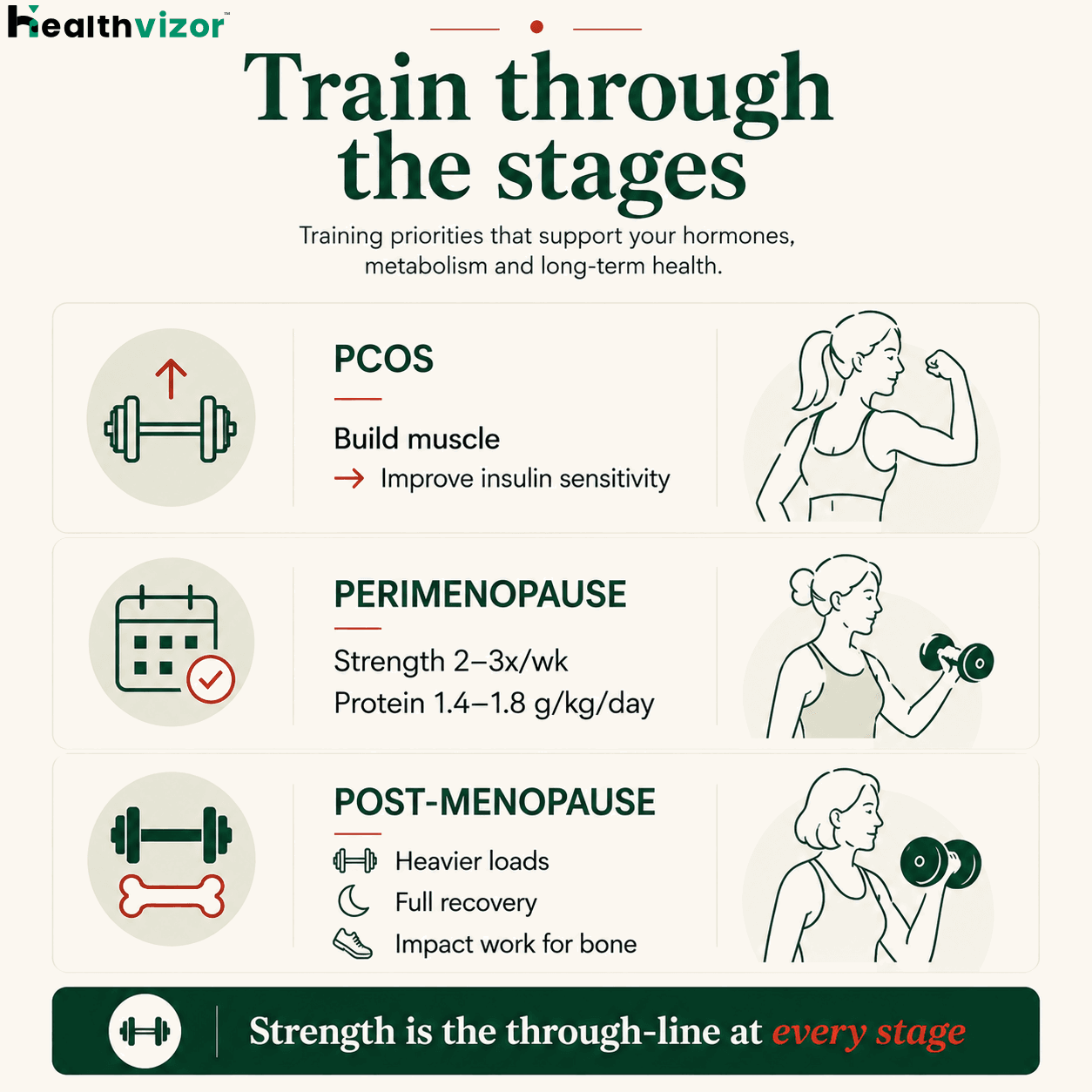
Training through PCOS
Strength training is the single most underused PCOS intervention. Building muscle improves insulin sensitivity and shifts body composition in a way pure cardio rarely matches in this group. Two to three resistance sessions a week, paired with some zone-2 cardio, beats long cardio-only routines for most women with PCOS.
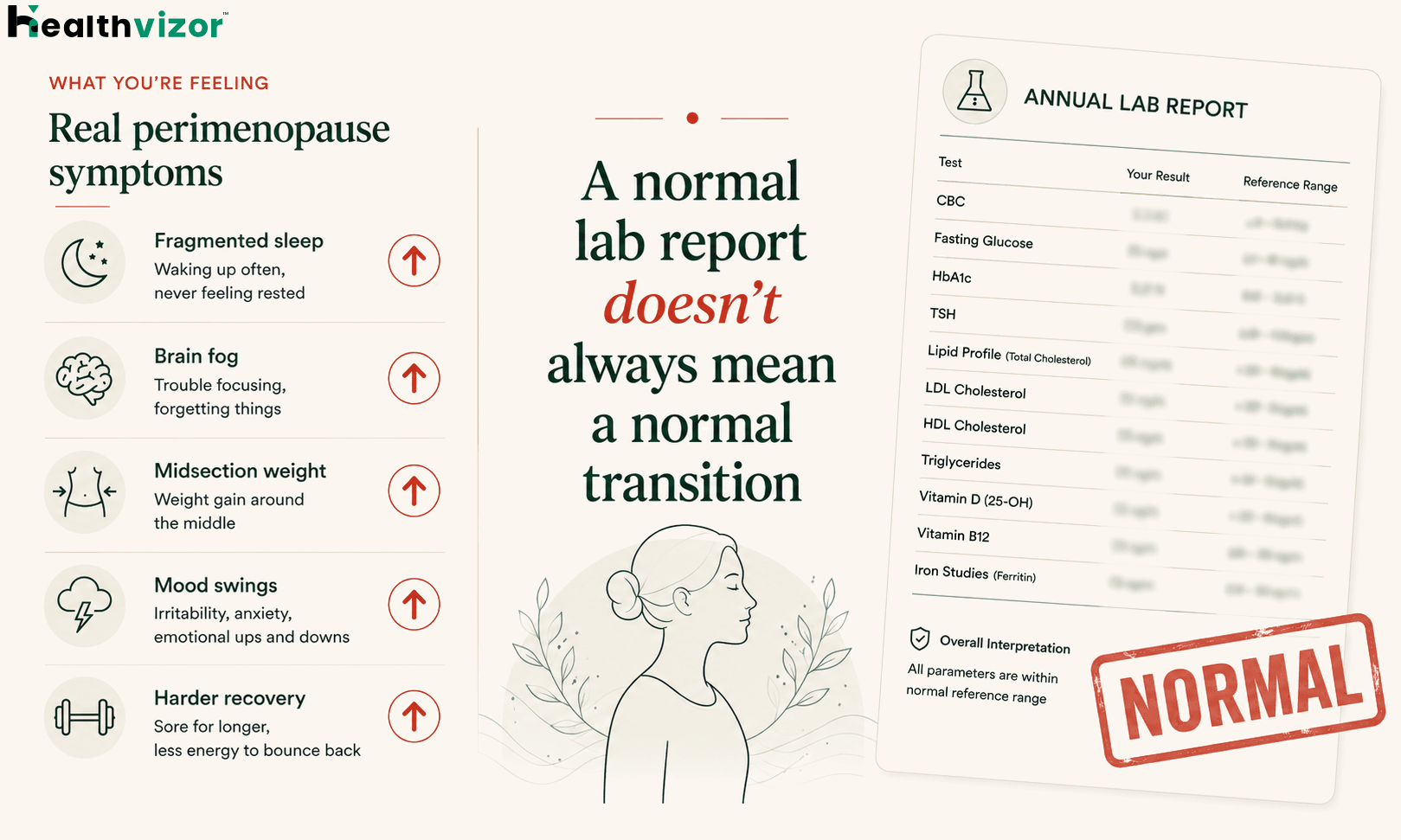
Stage 2: Perimenopause (the missing decade)
What changes in your biomarker map
FSH starts to rise as the pituitary works harder. A single value isn't diagnostic; the trend across cycles is what matters.
Estradiol turns erratic, high spikes, deep troughs. Symptoms often track the fluctuation, not the absolute level.
Progesterone drops earliest, feeding anxiety, poor sleep and heavier cycles.
ApoB and LDL start trending up as estrogen falls, the most under-discussed cardiovascular shift in women's health.
Fasting insulin and HOMA-IR drift upward, even at stable weight.
Vitamin D and B12 matter more, since both affect mood and energy when both are already strained.
Bone loss begins before menopause³. If you have risk factors, low body weight, a prior fracture, steroid use, early menopause, thyroid issues, low vitamin D, or a family history of osteoporosis, it's worth discussing a baseline DEXA with your doctor rather than waiting.
What works
Strength training, two to three times a week. This is the anchor, it protects muscle, bone and insulin sensitivity through the transition.
Protein: most women under-eat it. For active women, roughly 1.4–1.8 g per kg of body weight per day, spread across meals, is a sensible target.
Sleep becomes non-negotiable. Perimenopausal sleep is fragile; small changes (cooler room, less alcohol, magnesium glycinate at night) add up.
Hormone therapy is back on the table, thoughtfully. Modern menopause hormone therapy is far more nuanced than the post-WHI fear cycle. For the right woman, started near menopause, especially with non-oral estrogen routes, it can meaningfully improve symptoms and may carry a more favourable risk profile⁴'⁵. It is not a DIY supplement decision: have the conversation with a hormone-literate gynaecologist or endocrinologist.
Stage 3: Post-menopause
Post-menopause isn't "perimenopause, slower." It's a distinct cardiometabolic stage. Estrogen's protection against heart disease is gone. ApoB, LDL and triglycerides rise. Bone loss continues, fastest in the first five years. Visceral fat tends to climb even without weight gain. Cardiovascular risk catches up to, and eventually passes, that of male peers.
The SWAN study and later menopause-cardiovascular reviews show that the transition itself, independent of age, drives adverse changes in lipids, insulin sensitivity and inflammation³'⁴. So "I'm not gaining weight, why are my labs worse?" has a clear hormonal answer.
Biomarkers and intervals
Cardiac: ApoB, Lp(a) once, lipid panel, hs-CRP, homocysteine, annually.
Metabolic: HbA1c, fasting insulin, HOMA-IR, annually.
Bone: a DEXA baseline around menopause if you have risk factors, and screening for all women by age 65; repeat interval guided by your result. Add vitamin D, calcium and parathyroid hormone if vitamin D is low.
Hormonal: FSH, LH, estradiol, testosterone, SHBG once post-menopause, most useful if symptoms are bothersome or HRT is on the table.
Thyroid: full panel annually, subclinical hypothyroidism is more common in this age band.
Training after menopause
Cycle tracking is the missing skill
Most Indian women were never taught to map their cycle systematically, yet it's the foundational skill for managing PCOS and reading perimenopause. Track cycle length, bleeding, ovulation signs (cervical mucus, basal body temperature, LH strips), energy and mood across the month, training response and sleep. Apps like Clue and Flo are available on the Indian App Store and Google Play, use them for patterns, not diagnosis. Within three cycles, patterns emerge, and those patterns are what make lab results meaningful. A one-off FSH or estradiol with no cycle context is information without meaning.
Training with your cycle
Emerging (still mixed) evidence suggests strength gains may be slightly enhanced in the follicular phase (from your period through ovulation), while the luteal phase (after ovulation) brings higher core temperature, fluid retention and a higher recovery cost. Practical takeaway: put your heaviest sessions in the follicular phase when you can, and treat the late luteal week as higher-recovery. It's not about training less, it's about working with the biology. In perimenopause, cycle variability gets too high to plan rigidly, so you shift to training by feel and HRV trend.
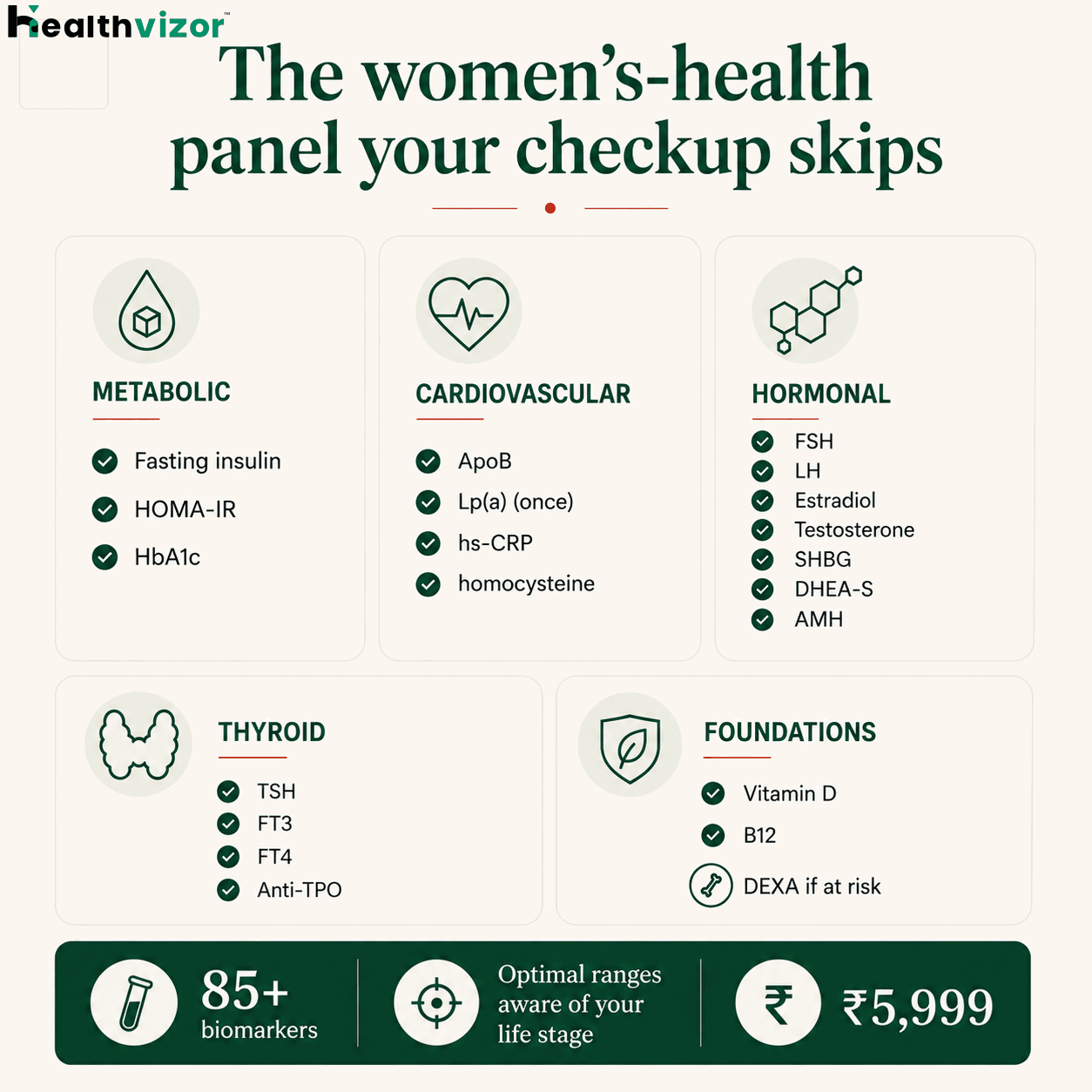
Healthvizor's 85+ biomarker panel covers the full women's-health stack at every stage, fasting insulin and HOMA-IR, lipids with ApoB and Lp(a), full thyroid (TSH, FT3, FT4, Anti-TPO), sex hormones (FSH, LH, estradiol, testosterone, SHBG, DHEA-S), AMH, vitamin D, B12, hs-CRP and homocysteine, each read against optimal ranges that are aware of where you are in your reproductive life. Your personalised plan changes depending on whether you're managing PCOS, navigating perimenopause, or protecting your heart and bones after menopause. Whichever stage you're in, your biology is doing something specific, and you deserve to see it clearly, not be told to wait until it becomes a diagnosis.
Frequently Asked Questions
Hormonal and metabolic changes often begin years before noticeable symptoms appear. Women with PCOS, a family history of diabetes or cardiovascular disease, or persistent symptoms such as fatigue, irregular cycles, or unexplained weight changes may benefit from earlier biomarker tracking under medical guidance.
Not always. Standard health checkups are designed to detect disease, but they may not identify early metabolic or hormonal shifts. Looking at trends across biomarkers over time often provides more meaningful insights than a single test result.
Insulin resistance markers such as fasting insulin and HOMA-IR, along with HbA1c, ApoB, lipid profile, testosterone, SHBG, DHEA-S, thyroid markers, vitamin D, and inflammatory markers like hs-CRP, can provide a broader picture of metabolic and hormonal health.
Yes. While no single test can diagnose perimenopause, tracking biomarkers alongside symptoms over time can help identify changes in metabolism, cardiovascular health, bone health, and hormonal patterns that occur during the transition.
After menopause, cardiovascular risk, insulin resistance, and bone loss become increasingly important. Regular monitoring of metabolic, cardiovascular, thyroid, and bone-related biomarkers can help guide preventive care.